
Shoulder Pain and Chiropractic

Shoulder pain is very common, and according to Urwin et al. (1) between 16% to 26% of the population will experience it at some time.
Shoulder pain can be disabling and result in compromised shoulder movements due to pain, stiffness or weakness, which has an effect on everyday activities such as getting dressed, eating, work etc.
Urwin et al. state that it is the third most common cause of musculoskeletal consultations in primary care.
The shoulder is a very complex joint surrounded by many ligaments and muscles that work to coordinate its' movement and the surrounding joints. The shoulder is a very mobile joint so relies heavily on the fine coordination of it's muscles to work correctly, and therefore cannot always provide the stability needed for certain movements. Many shoulder injuries result in more than one structure becoming dysfunctional or painful.
Common causes of shoulder pain
- Instability (traumatic or non traumatic)
- Impingement syndrome
- Tendonitis or bursitis
- Osteoarthritis
- Adhesive Capsulitis (Frozen Shoulder)
- Acromioclavicular joint separation
- Referred pain from Cervical Spine
- Partial or full tears of tendons/muscles
- Fracture following trauma
- Muscles strains or ligament sprains
- Poor posture
- Overuse
Other causes which are less common are:
- Visceral (organ) referral pain
- Tumour
- Infection
- Calcification of bursae or tendons
NB The above lists are not all inclusive and there can be other causes of shoulder pain. If the Chiropractor feels it is necessary they may refer for further investigation such as X-ray, ultrasound imaging, GP etc to reach an accurate diagnosis.
How can Chiropractic help?

Your chiropractor will carry out a detailed case history and carry out an examination to determine the cause of pain. If required you may be referred for further investigation such as X-rays - to assess the joints; MRI - to assess the soft tissue structures such as ligaments and tendons; ultrasound - to assess joint, ligament and tendons; or blood tests - to test for medical conditions.
Once a diagnosis has been reached, if it is musculoskeletal, your Chiropractor can offer a range of treatment options such as joint manipulation or mobilization, soft tissue treatments such as trigger point therapy or acupuncture. Along with home care/ergonomic advice and rehabilitation programmes.
Shoulder Anatomy
The shoulder is one of the most mobile joints in the body, it's only bony connection is where the clavicle connects with the sternum (chest bone) so it relies heavily on the surrounding muscles and ligaments for stability. Any damage or dysfunction in any of the stabilizers causes high demands on the other supporting structures to maintain the joint flexibility and movements.
The shoulder provides the arm with a wide range of motion - flexion, extension, abduction, adduction, internal and external rotation. The shoulder also allows for movement of the scapula, such as protraction, retraction, elevation and depression.
Bone Structures
The shoulder joint consists of: the humerus (upper arm), the scapula (shoulder blade) and the clavicle (collar bone).
The clavicle connects with the sternum (chest bone), creating the sternoclavicular joint; and then with the acromion of the scapula laterally creating the acromioclavicular joint.
To the front of the scapula there is a projection of the scapula called the coracoid which is an attachment point for muscles and ligaments.
On the scapula the Glenohumeral Fossa is the socket where the head of the humerus sits, forming the ball and socket joint. It is held in place with the assistance of ligaments, and the rotator cuff muscles.
The glenoid labrum deepens the fossa (socket) providing more stability to the joint.
Extrinsic (superficial) Muscles
Anterior muscle:
- Pectoralis Major - The pectoralis major has four actions. The first is flexion of the humerus, it also adducts the humerus, rotates the humerus medially, and keeps the arm attached to the trunk of the body.
Posterior muscles:
- Trapezius - elevates shoulder and rotates scapula to extend upwards.
- Latissimus Dorsi - Extends, adducts and internally rotates arm; draws shoulder inferiorly and posteriorly; keeps inferior angle of scapula against chest wall
Lateral Muscles:
- Deltoid muscles are in 3 compartments: Anterior - flexes and internally rotates arm; middle - abducts arm and posterior - extends and externally rotates arm. The deltoids take over when the arm is lifted away from the body.
Intrinsic (Deep) Muscles
Anterior muscles:
- Pectoralis Minor - draws scapular anteriorly and internally, raises rib in forced inspiration.
- Subclavius - depresses clavicle, draws shoulder anteriorly and inferiorly, steadies clavicle during movements of shoulder girdle.
Posterior Muscles:
- Levator Scapula - Elevates scapula, and rotates or extends the neck when the scapular is fixed in position.
- Rhomboid major and minor - retract and elevate scapula.
- Teres major - extends and internally rotates humerus.
Lateral Muscles:
- Serratus Anterior- pulls scapula anterior of the thoracic wall and rotates scapula for abduction and flexion of the arm
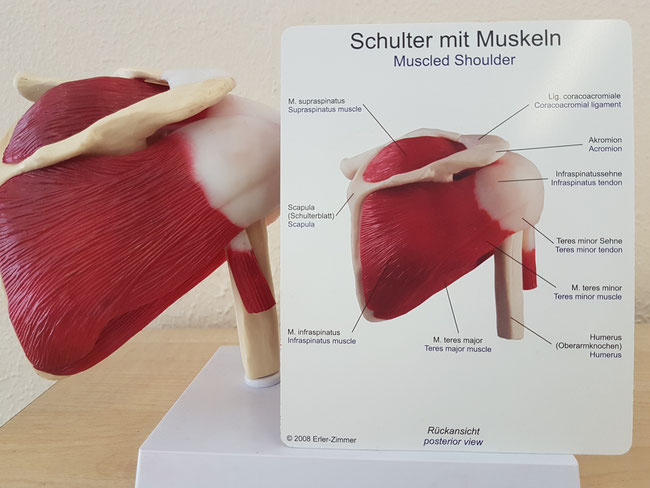
Rotator Cuff Muscles:
- Supraspinatus - flexes arm, aids deltoid abduction, draws humerus towards glenoid fossa, prevents deltoid forcing humerus up against acromion.
- Infraspinatus - draws humerus towards Glenoid Fossa, resisting posterior dislocation of arm, externally rotating and abducting arm.
- Teres Minor - externally rotating arm and assists with minimal adduction of arm.
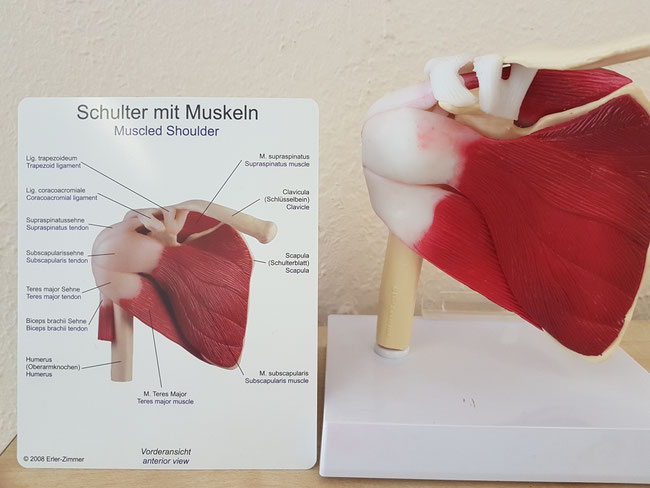
- Subscapularis - internally rotates arm and stabilizes glenohumeral (shoulder) joint.
Muscles of shoulder and arm
- Biceps Brachii - consists of two heads: long head and short head. Primary flexor of forearm, supinates forearm and weakly flexes the arms at shoulder.
- Coracobrachialis - weakly adducts arm and aids with stabilizing the humerus
- Triceps brachii - consists of three heads. Primary extensor of forearm at elbow joint, long head crosses glenohumeral joint so it can also extend and adduct humerus.
Shoulder Bursae
Bursae are fluid filled sacs, found between two moving surfaces to allow the surfaces to move freely and reduce friction between structures. Inflammation of a bursa is called Bursitis.
Shoulder Ligaments
There are various ligaments around the shoulder joint to provide stability, they include:
- Glenohumeral Ligament
- Coraco-acromial ligament
- Coraco-clavicular ligament
- Transverse Humeral Ligament
Mitchell et all (2,) carried out a study of Shoulder Pain: diagnosis and management in primary care. They concluded the following:
"Shoulder pain is a common and important musculoskeletal problem. Management should be multidisciplinary and include self help advice, analgesics, relative rest, and access to physiotherapy. Steroid injections have a marginal short term effect on pain.
Poorer prognosis is associated with increasing age, female sex, severe or recurrent symptoms at presentation, and associated neck pain. Mild trauma or overuse before onset of pain, early presentation, and acute onset have a more favourable prognosis (3,4). No evidence exists to show that early orthopaedic intervention improves the prognosis for most rotator cuff or glenohumeral disorders. Surgery should be considered when conservative measures fail."
NB Please note that the above is not applicable to everyone. If you have any questions then please contact us to discuss further.
References
1.Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis 1998;57: 649-55.
2. Mitchell C, Adebajo A, Hay E, Carr A. Shoulder pain: diagnosis and management in primary care. BMJ : British Medical Journal. 2005;331(7525):1124-1128.
3. Van der Windt DA, Koes BW, Boeke AJ, Deville W, De Jong BA, Bouter LM. Shoulder disorders in general practice: prognostic indicators of outcome. Br J Gen Pract 1996;46: 519-23.
4.Thomas E, van der Windt DA, Hay EM, Smidt N, Dziedzic K, Bouter LM, et al. Two pragmatic trials of treatment for shoulder disorders in primary care: generalisability, course, and prognostic indicators. Ann Rheum Dis 2005;64: 1056-61.
Write a comment
lxbfYeaa (Tuesday, 02 August 2022 12:40)
20
lxbfYeaa (Tuesday, 02 August 2022 12:41)
20
lxbfYeaa (Tuesday, 02 August 2022 13:36)
20
lxbfYeaa (Tuesday, 02 August 2022 13:36)
20
lxbfYeaa (Tuesday, 02 August 2022 13:43)
20
lxbfYeaa (Tuesday, 02 August 2022 13:43)
20
lxbfYeaa (Tuesday, 02 August 2022 14:36)
20
lxbfYeaa (Tuesday, 02 August 2022 14:37)
20
lxbfYeaa (Tuesday, 02 August 2022 15:28)
20
lxbfYeaa (Tuesday, 02 August 2022 15:29)
20